2.8.1
Correction of dental-alveolar lengthening
Correction of dental-alveolar lengthening Correction of dental-alveolar lengthening Correction of dental-alveolar lengthening Correction of dental-alveolar lengthening Correction of dental-alveolar lengthening Correction of dental-alveolar lengthening Correction of dental-alveolar lengthening
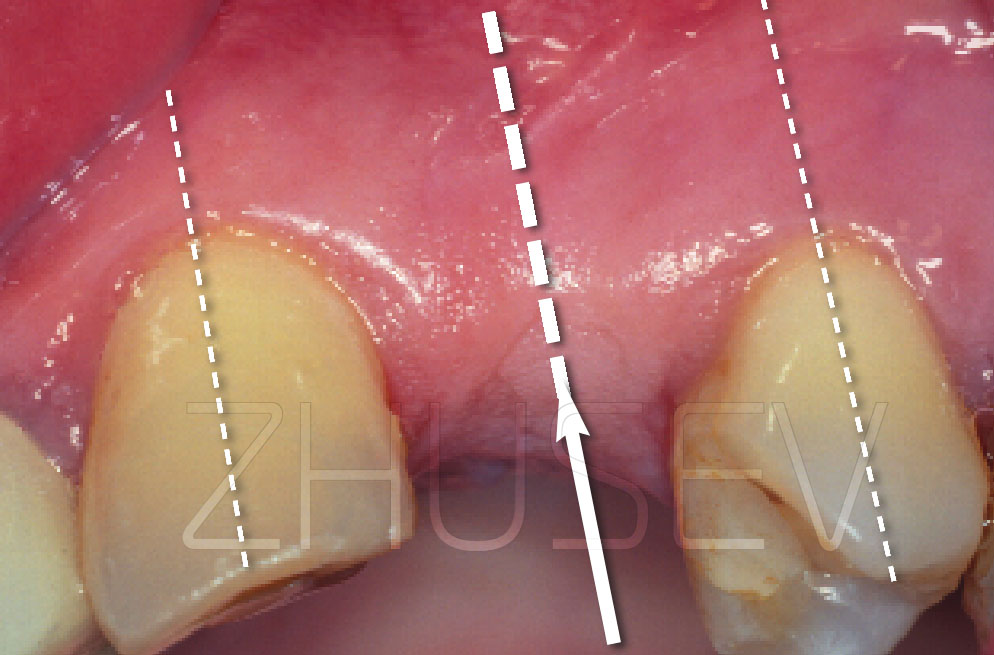
Rather commonly, the bone volume for the installation of implants is sufficient, but teeth that have advanced due to the Popov-Godon phenomenon (dento-alveolar lengthening) in the opposite jaw do not allow to make an orthopedic structure, and simple preparation of the advanced teeth in height will sharply reduce the level of cement fixation for the crowns; and the crowns themselves will be too short (2.8.1-1A) and, as a result, unesthetic.
In such cases, you can perform a simple operation that will solve these problems. It is important that the supporting teeth should be stable and have long roots without symptoms of inflammation.
2.8.1-1A We do implantation in the lower jaw. In the upper one, there is an orthopedic construction that will frequently lose cement. The teeth have been drilled so much that the area of cementation is dramatically reduced.
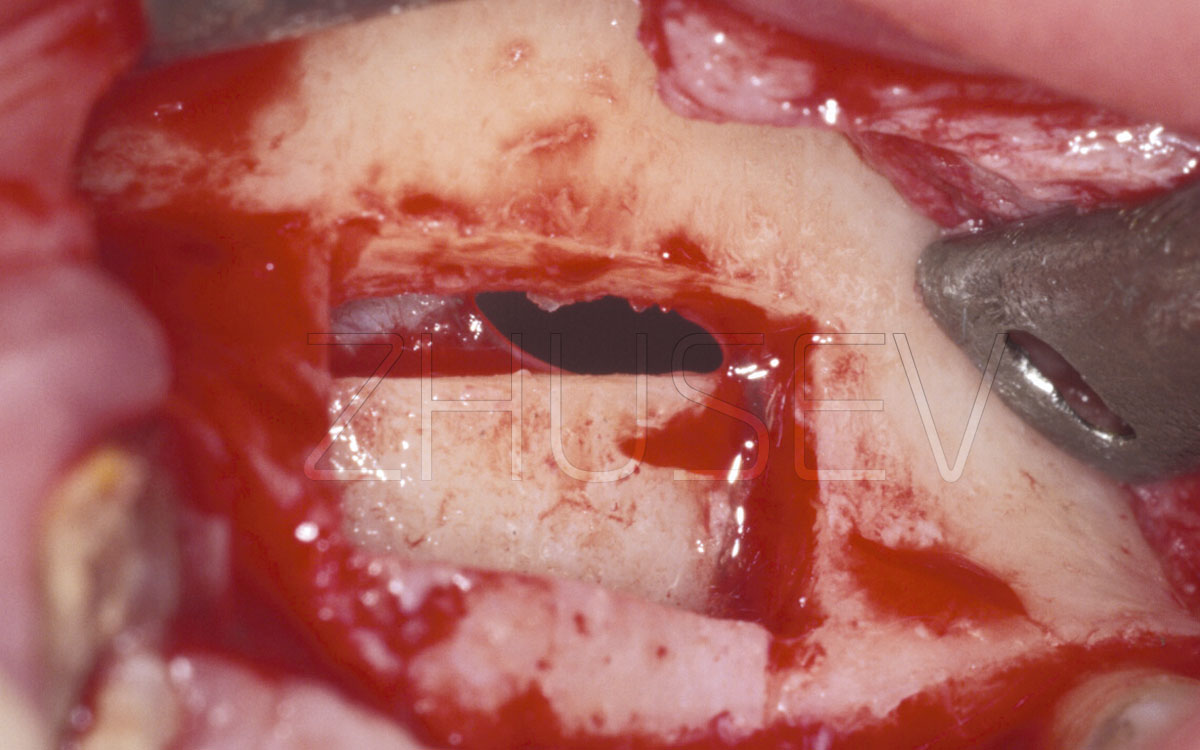
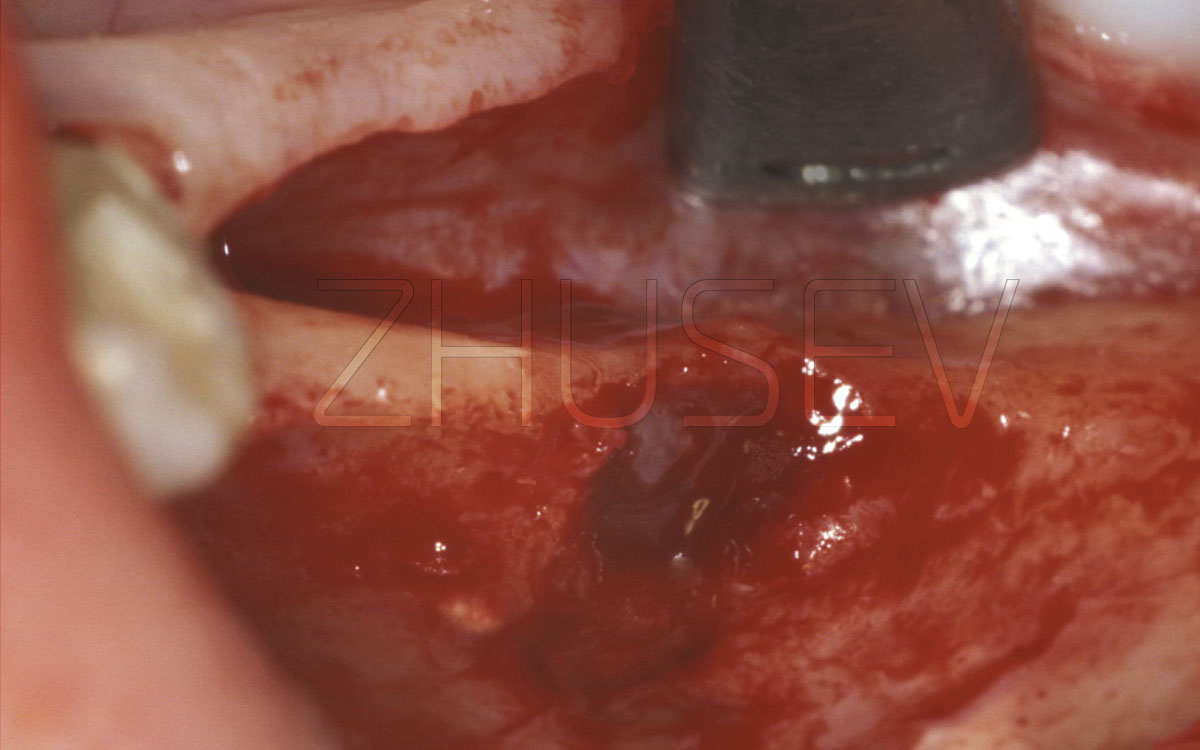
2.8.1-1B We unfold the mucoperiosteal flap. At the same time, gently lift it at the teeth that limit the defect (in this case, it is tooth 13).
If it is clear that the advanced teeth will have to be intensively milled, they should be depulped before the operation.
If this operation is carried out in an esthetically important area, then it is necessary to make temporary plastic crowns to form a marginal edge. Be careful when fixing these crowns! Superfluous cement can easily penetrate the gum (still fragile) and cause inflammation. Therefore reduce the amount of temporary cement to a minimum.
Following the surgery, tell the patient to apply dental Solcoseryl 3-4 times a day (best after each meal) for 7-10 days. Repeat this series after fixing the temporary crowns.
With all its apparent complexity, the operation is really simple and seriously expands the possibilities of joint fruitful work of the surgeon and the orthopedist. Obviously, it can be used not only for implantations.
2.8.1-1C We cut off 2-3 mm of the interdental partitions and of the cortical plate with the Lindemann drill, trying not to damage the dentin of the teeth roots. You should by no means remove the remaining fragments of the epithelium between the teeth.
2.8.1-1D Return the mucoperiosteal flaps to their initial location, and check the level of exposed teeth: if this is insufficient, we perform additional gingivotomy.
2.8.1-1E Following the shape of the flap, cut the excesses. It is important that when suturing flaps should lie down without excessive tension or folds. We see recovery of the fixing height and the general smile curve.
2.8.1-1F
We cover all wounded surfaces with dental Solcoseryl.
2.8.1-1G
14 days after the operation, temporary plastic crowns were manufactured and installed. This a view 2 months after surgery. A week later, the implants were installed on the lower jaw.
2.8.1-1H
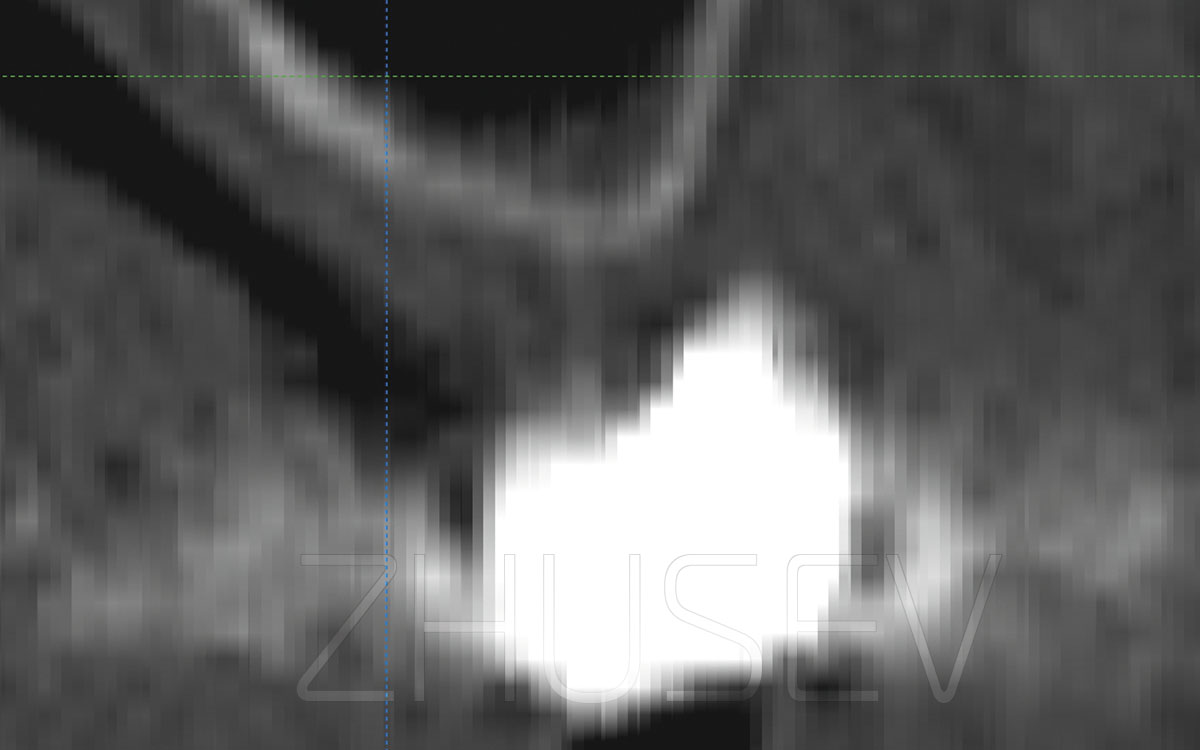
Reference X-ray taken 2 months after the implantation. In the osteotomy area of the upper jaw we observe minimal bone loss!
2.8.1-1I
Orthopedic work is completed. The clinical height of crowns is restored and reliable cement fixation is provided.